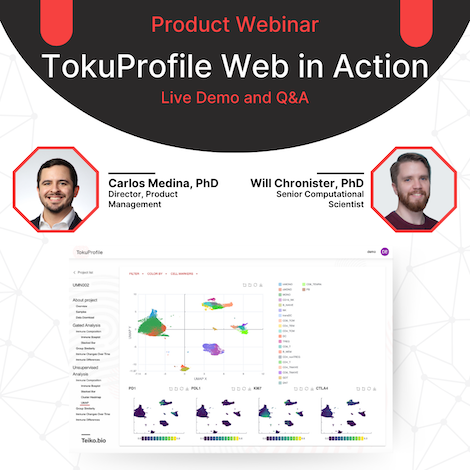
In this live webinar, Carlos Medina, Director of Product Management, and Will Chronister, Senior Computational Scientist, demonstrate how the newly redesigned TokuProfile Web can be used to answer critical research questions. This live demo will uses a real-world customer dataset, graciously provided by Dr. Shernan Holtan, Associate Professor at the University of Minnesota.
About the Speakers
Prior to Teiko, Carlos Medina completed his PhD training in Immunology at Stanford University in the laboratory of Dr. Paul Bollyky. There, he investigated the impact of the tissue extracellular matrix on regulatory T cell subsets in autoimmune diabetes and allergic asthma. Carlos has extensive experience in cytometry and immune cell profiling across a wide range of disease models.
Prior to Teiko, Will Chronister completed his PhD training in Biochemistry and Molecular Genetics at the University of Virginia. There, he investigated brain somatic mosaicism using single cell analysis and whole genome sequencing. Following this, he held roles as a Postdoctoral Fellow at the La Jolla Institute for Immunology and then as a Scientist, Bioinformatics at Fate Therapeutics before joining Teiko in early 2023.
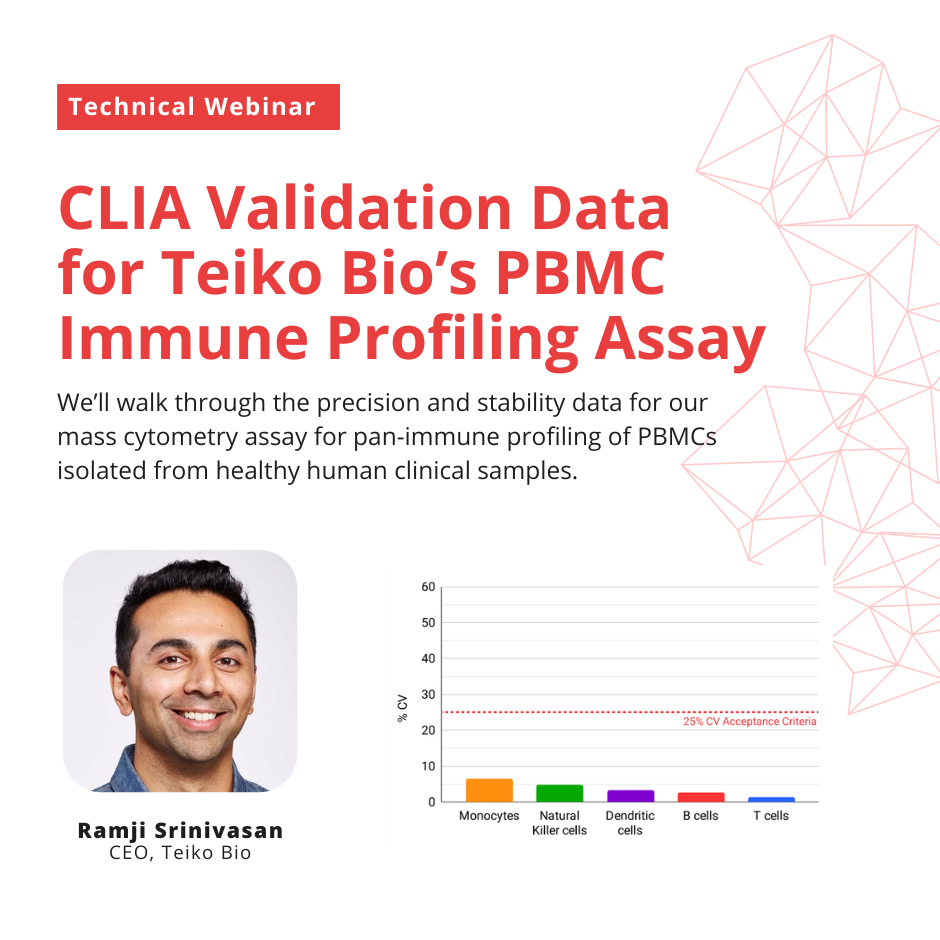
In this live webinar, Ramji Srinivasan, cofounder and CEO of Teiko Bio, will walk through the precision and stability data for our mass cytometry assay for pan-immune profiling of PBMCs isolated from healthy human clinical samples.
About the Speaker
Before Teiko, Ramji was Cofounder, CEO and Chairman of Counsyl, a women’s health genetic screening laboratory. Counsyl screened over 1M prospective parents, mothers-to-be and women at risk of hereditary cancer. In 2018, Counsyl was acquired by Myriad Genetics, Inc for $375M in cash and stock.
Ramji earned a B.S. in computer science and an M.S. in financial mathematics, both from Stanford University. Ramji also attended Stanford’s Graduate School of Business before dropping out to start Counsyl.
In this technical webinar, Jolien Sweere, PhD, discusses data from a technical validation experiment performed by Teiko Bio showing how mass cytometry immune profiling data from whole blood compares to data from PBMCs.
Jolien Sweere, PhD completed her doctoral training in Immunology at Stanford University in the laboratory of Paul Bollyky. During her PhD, she found that a type of temperate filamentous bacteriophage that infects Pseudomonas aeruginosa is associated with chronic human wound infections. Her work was published in Science in 2019.
After completing her PhD, Jolien worked as a Life Sciences commercial strategy consultant at Charles River Associates in San Francisco. She joined Teiko Bio in 2022 as a Senior Scientist, Medical Strategy.
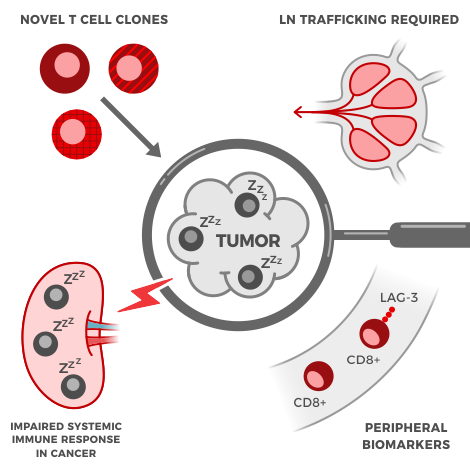
About ~40-60%[1] of first-line metastatic melanoma patients receive immunotherapy. But depending on the type of treatment, between 15-50% of those patients will have a severe immune-related adverse event of grade 3 or higher. These aren’t headaches either; the adverse events are serious, like Grade 3 hepatitis or colitis. These kinds of events “interfere with a person’s ability to do basic things like eat or get dressed.”[2] The problem is, drug developers and doctors don’t know which kind of patients will experience these adverse events. That’s why we’re attempting to crack this problem, by looking at immune signatures found in the blood of melanoma patients.
In this recorded live webinar, Ramji Srinivasan, cofounder and CEO of Teiko Bio, shares original research on blood-based biomarkers of immune-related adverse events in metastatic melanoma performed by Teiko scientists in collaboration with Dr. Siwen Hu-Lieskovan of Huntsman Cancer Institute.
About the Speaker
Before Teiko, Ramji was Cofounder, CEO and Chairman of Counsyl, a women’s health genetic screening laboratory. Counsyl screened over 1M prospective parents, mothers-to-be and women at risk of hereditary cancer. In 2018, Counsyl was acquired by Myriad Genetics, Inc for $375M in cash and stock.
Ramji earned a B.S. in computer science and an M.S. in financial mathematics, both from Stanford University. Ramji also attended Stanford’s Graduate School of Business before dropping out to start Counsyl.
Immunotherapies work solely by activating immune cells within the tumor – or do they? In this webinar, Dr. Jolien Sweere walks us through a number of scientific studies published within the last 6 years showing that immune responses outside the tumor are necessary for effective immunotherapy. She also highlights more recent work, including work done by Teiko Bio, that found peripheral immune features associated with improved clinical outcomes and presentation of immune related adverse events.
About the Speaker
Jolien Sweere, PhD completed her doctoral training in Immunology at Stanford University in the laboratory of Paul Bollyky. During her PhD, she found that a type of temperate filamentous bacteriophage that infects Pseudomonas aeruginosa is associated with chronic human wound infections. Her work was published in Science in 2019.
After completing her PhD, Jolien worked as a Life Sciences commercial strategy consultant at Charles River Associates in San Francisco. She joined Teiko Bio in 2022 as a Senior Scientist, Medical Strategy.
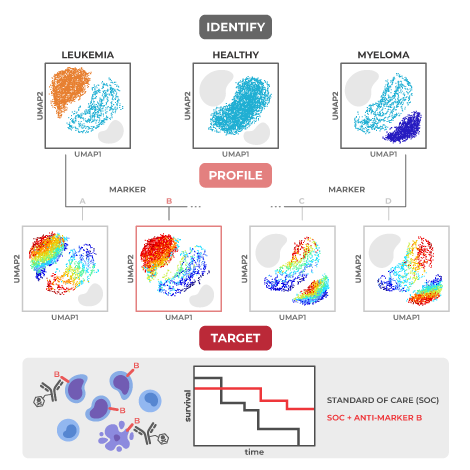
Many blood cancer studies today use immune profiling detection platforms that simply count the number of cancer cells, without providing any detailed information about their characteristics or interactions with healthy immune cells. This is where mass cytometry comes in – with the ability to evaluate over 40 protein markers per cell across hundreds of thousands of cells per blood sample1, it provides high-dimensional data that researchers can use to make crucial therapeutic discoveries.
Here, we highlight six recent key discoveries made using mass cytometry across a wide range of blood cancers including acute myeloid leukemia (AML), acute lymphoid leukemia (ALL), large B cell lymphoma, and multiple myeloma. With this powerful tool, researchers have uncovered new mechanisms of cancer relapse after chemotherapy, identified predictive biomarkers of response, and disentangled the role of non-cancerous immune cell populations in blood-based cancers.
High rate of dysfunctional NK cell development predicts poor outcomes in acute myeloid leukemia (AML)
Published in PNAS in 2021, Chretien et al. used two ~30 marker mass cytometry panels to characterize ‘dysfunctional’ natural killer (NK) cells overrepresented in newly diagnosed AML patients relative to healthy controls. This ‘dysfunctional’ NK population lacks expression of CD56, a marker highly associated with NK function, but expresses CD16, a crucial marker for antibody mediated killing by NK cells (CD56-CD16+).2 Importantly the cytotoxic killing potential of these cells, measured by degranulation in response to target cells, is reduced.
The authors found that having a higher percentage of these CD56- CD16+ NK cells at diagnosis was associated with poor clinical outcomes, lower overall survival, and a reduced likelihood of living free from disease complications (event-free survival). High dimensional analysis of single-cell protein expression by mass cytometry showed that these cells have lower expression of five activating receptors important for NK cytotoxic function: NKp30, NKp46, NKG2D, DNAM-1, and CD96.
Using an algorithm to analyze developmental pathways, the authors were able to identify a branching-off point where normal, mature NK cells diverge to become these dysfunctional NK cells. Future therapeutics targeting NK cells at this developmental stage may restore developmentally mature, functional NK cell populations for patients with AML, and thus likely improve clinical outcomes.
AML FLT3-ITD mutation and chemotherapy response: Why cytarabine might not be the best option
A study by Rörby et al. published in late 2021 used mass cytometry to approach the question: how does PKC412 synergize with a current standard chemotherapy regimen to produce good responses in AML patients?3 PKC412 is a newer anti-cancer drug, also called midostaurin, that improves overall survival for AML patients treated with a standard chemotherapy regimen consisting of daunorubicin and cytarabine. In 2017, it received approval by the US Food and Drug Administration (FDA) for use in patients with newly diagnosed FLT3-mutated AML, which is a common mutation affecting a third of AML patients that carries a poor prognosis. The researchers wanted to parse out the mechanism behind PKC412’s synergy with standard chemotherapy in order to potentially achieve higher clinical response rates by boosting complementary pathways and eliminating antagonist ones.
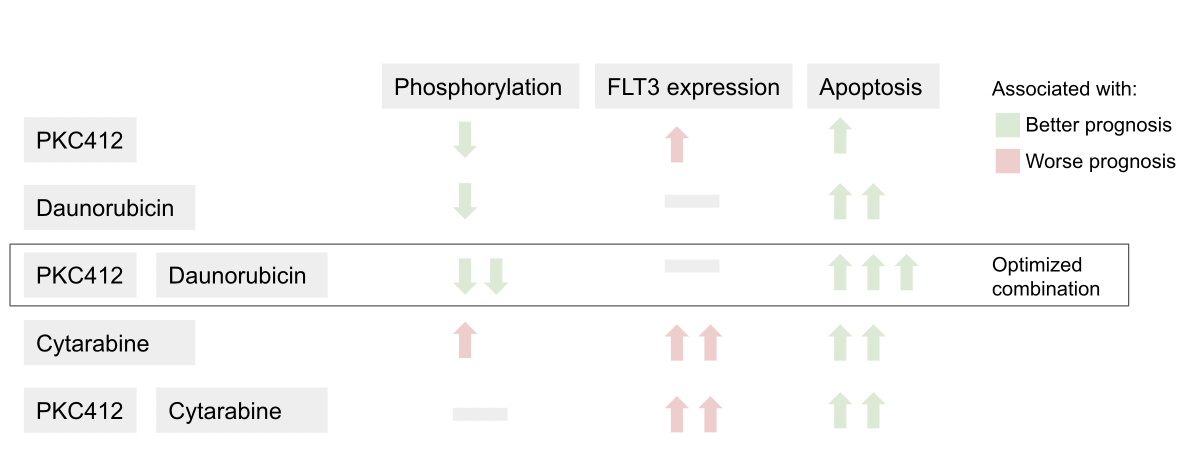
To tease out the impact of PKC412 on each component of the conventional treatment regimen, Rörby et al. used a 37-marker mass cytometry panel to evaluate the effects of various combinations of PKC412, daunorubicin, and cytarabine on intracellular signaling.
Summary of the effects of each drug combination on cell state
The authors found that daunorubicin works in concert with PKC412 to reduce phosphorylation (the addition of a phosphate group), a process that is necessary for molecular signaling cascades.3 In contrast, cytarabine increases FLT3 cell membrane receptor expression and intracellular signaling that reverses the activity of PKC412. These findings suggest that chemotherapeutic regimens without cytarabine, such as daunorubicin plus PKC412, may be more effective in treating the many AML patients who carry the FLT3-ITD mutation.
A combinatorial biomarker is a better predictor of response to anti-CD22 than CD22 expression alone in acute lymphoblastic leukemia (ALL)
With standard of care, around 90% of pediatric acute lymphoblastic leukemia (ALL) can be cured, but there is still around 10% of pediatric patients with relapsed or refractory (R/R) disease that remain resistant to treatment.4 A new drug that shows great potential to treat those with R/R ALL is Inotuzumab ozogamicin (InO), a CD22-directed antibody-drug conjugate. Although research from the Children’s Oncology Group and others suggested that resistance to InO might occur via reduced CD22 protein expression or density on the cell membrane, biomarkers for response to InO treatment had never been directly investigated.5
Diaz-Flores et al. used mass cytometry to evaluate whether the expression of any combination of 35 rationally selected protein antigens was associated with treatment response to InO.4 The proteins selected included cell surface markers, intracellular signaling molecules, and anti-apoptotic (cell survival) proteins that prevent programmed cell death, as well as other markers known to prevent cancer (so-called tumor suppressors) or resist drug exposure. After comparing antigen expression at diagnosis to changes in antigen expression after one and two cycles of treatment using a high-dimensional tumor cell-community clustering algorithm, the researchers were able to identify important combinatorial biomarkers predicting response to treatment.
The study authors identified the antigens that played the greatest role in distinguishing between complete and partial responder patient groups. Out of the handful of antigens identified, the most important discovery from the study was that low levels of CD22 had to be coupled with high levels of Bcl-2, an anti-apoptotic protein, to predict poor response to treatment. Low levels of CD22 alone could not predict poor response. These results suggested that the effects of InO, a drug that targets CD22, could possibly be improved by combining it with a drug to inhibit Bcl-2.
Exhausted NK cells hold the key to Daratumumab resistance in multiple myeloma (MM)
A study by Verkleij et al. used both flow and mass cytometry to evaluate the cellular response to the drug Daratumumab (DARA) in both newly diagnosed and relapsed/refractory multiple myeloma (R/RMM) patients.6 DARA, as part of a chemotherapy regimen, has been a promising treatment for R/RMM, with another study showing an improvement in complete response by 10% with the addition of DARA to a standard chemotherapy regimen.7 In this study, Verkleij et al. analyzed over 30 patient bone marrow and peripheral blood samples at baseline and at relapse using a mass cytometry panel with 39 surface and intracellular markers.
The authors found greater numbers of NK cells with an exhausted phenotype (higher frequency of TIM-3 expression and lower frequency of CD16 expression) in non-responding patients compared to responding patients at baseline, which was also seen in patients who relapsed. NK cells with an exhausted phenotype no longer carry out their normal characteristic functions such as the release of inflammatory signals or the ability to kill cancer cells. Patients with poor clinical outcomes also had greater numbers of both NK and T cells with an exhausted phenotype.
To determine whether resistance to DARA was due to NK cell exhaustion rather than a change in the multiple myeloma cancer cells themselves, the authors took cancer cells from patients who developed resistance to DARA and combined them with NK cells from healthy donors plus DARA treatment. They saw that DARA resistance was overcome by the addition of healthy NKs, suggesting that patients resistant to DARA may benefit from targeted reinvigoration of NK cells so they can destroy cancer cells again. This insight into the key role of NK cell activity was made possible by large-scale immune profiling through mass cytometry and is broadly applicable to situations where the target immune cell is initially unknown.
Tracking the success of CAR T cell therapy in MM with peripheral blood CD8+ T cells
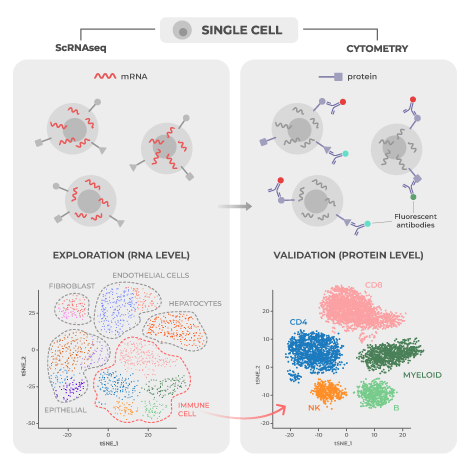
Another promising treatment for R/RMM is B cell maturation antigen (BCMA) CAR-T cell therapy, which involves genetically engineering a patient’s T cells so that they respond more forcefully to combat cancer cells. While many patients respond well to therapy, the response can be quite variable both in terms of initial effectiveness and in the duration of benefit. To explore variables that predict how patients will respond to BCMA CAR-T cell therapy, Melnekoff et al. conducted a study assessing single-cell transcriptomic and proteomic data from bone marrow (which is the tumor microenvironment in multiple myeloma) and peripheral blood samples using mass cytometry and single-cell RNA sequencing (scRNA-seq).8, two complementary technologies.
Using a mass cytometry panel of 39 cell markers, study authors analyzed 3.5 million peripheral blood mononuclear cells (PBMCs) from 11 patients treated with BCMA CAR-T cell therapy. Analysis of samples taken from peripheral blood and the bone marrow tumor microenvironment at baseline revealed that there were distinct cell population markers distinguishing good responders from poor responders, with responders having greater percentages of CD8+ T cells and lower percentages of CD14+ monocytes in both peripheral blood and bone marrow and lower NK cell population percentages in peripheral blood.
These same population changes were also observed over time in response to expansion of CAR-T cells in patients. Comparing week 0 to week 4 on CAR-T therapy, non-engineered CD8+ T cell numbers increased while CD14+ monocyte numbers decreased. The non-engineered CD8+ T cells were found to be exhibiting a so-called “effector-memory” phenotype that enables an immediate robust immune response at the site of contact with the disease-carrying cells. These shifts reverse when a relapse on CAR-T therapy occurs. CD14+ monocyte numbers level off or increase and CD8+ T cell numbers decline. Melnekoff et al. concluded that a certain class of immunomodulatory drugs called immunomodulatory imide drugs might increase the effectiveness of CAR-T therapy by increasing natural CD8+ T cell numbers.
A unique population of post-infusion CAR Treg cells identify patients resistant to CD19-CAR therapy
Treating diffuse large B cell lymphoma (DLBCL) patients with axi-cel, a chimeric antigen receptor (CAR) T cell therapy targeting CD19 (an important B cell biomarker) has proven to be difficult, with lymphoma continuing to progress in around 60% of patients and neurological toxicity affecting two-thirds of patients.9 Biomarkers connected to poor disease control and neurotoxicity have not been well characterized. For this reason, Good et al. conducted a study to investigate circulating CAR T cells in 32 patients treated with axi-cel using mass cytometry to profile 37 proteins per cell.
The researchers found two metaclusters associated with complete response, both of which were positive for CD57 and expressed inhibitory proteins, such as PD-1, at lower levels.9 They also found a metacluster of CD4+Helios+ CAR T cells 7 days post-infusion that correlated with disease progression and diminished neurotoxicity. These cells expressed high levels of CD25, CTLA4 and TIGIT, a phenotype characteristic of immunosuppressive regulatory T cells (Tregs). The authors validated their findings in a prospective cohort analysis of 31 DLBCL patients treated with axi-cel.
This study demonstrates the usefulness of mass cytometry to find biomarkers correlated with treatment response, disease progression, or toxicity in DLBCL patients. The discovery of a unique population of CAR Treg cells associated with disease progression and reduced neurotoxicity may allow future researchers to specifically manipulate these cells before or after infusion to promote anti-tumor effect or lower neurotoxicity.
Future of high-dimensional immune profiling for blood cancers
In addition to the examples highlighted earlier, recent research presented at the December 2022 American Society of Hematology Conference investigated many other blood cancers, including follicular lymphoma and chronic myeloid leukemia. Other ongoing studies focus on AML patients with adverse cytogenetics and drug resistance in patients with other blood cancers like DLBCL and multiple myeloma.
Collectively, these studies showcase the capabilities of mass cytometry to identify peripheral immune biomarkers that can predict relapse and treatment response across a broad range of blood cancers. A recent pre-print by Kleftogiannis et al. does just this using a combination of mass cytometry and machine learning algorithms to identify predictors of survival in leukemia. The technology’s unique ability to profile both the patient’s tumor and immune cells at the single-cell protein level positions it as an excellent tool to unravel the mechanisms behind relapse and response. This deeper understanding of the disease can then inform the development of more effective treatment protocols and therapies.
In this educational webinar, Matthew Spitzer, PhD, reviews the current body of literature focused on answering the question “where do T cells get activated after cancer immunotherapy?” He also discusses his lab’s recent contribution in Cell (Rahim, Okholm, & Jones et al. 2023), which shows that successful T cell activation can be detected via peripheral blood immune profiling and that lymph node metastases can severely impair these processes. Read Teiko’s synopsis and highlights of Rahim, Okholm, & Jones et al. here.
About the Speaker
Matt Spitzer, PhD completed his training in Immunology at Stanford University in the laboratories of Garry Nolan and Edgar Engleman. There, he developed experimental and analytical methods to model the state of the immune system using high dimensional single-cell data. At Stanford, he also developed new strategies for inducing powerful immune responses against cancer.
Matt moved to UCSF in the summer of 2016 as a UCSF Parker Fellow and a Sandler Faculty Fellow and is now an Associate Professor in the Departments of Otolaryngology-Head and Neck Surgery and Microbiology & Immunology and an investigator of the Parker Institute for Cancer Immunotherapy. Matt is the scientific cofounder of Teiko Bio.
Everyone has a distinct “immune setpoint” that determines the way they respond to diseases and treatments. Matthew Spitzer, Associate Professor at UCSF and scientific cofounder of Teiko Bio, explains how understanding each patient’s individual immune setpoint could be the key to maximizing cancer treatment efficacy.
What is an “immune setpoint” and how does it affect our responses to life-threatening diseases like cancer?
Each individual’s immune system is characterized by a unique homeostatic baseline, called the immune setpoint. The immune setpoint defines how our immune system behaves naturally, in the absence of a disturbance. This is based on our underlying genetics, historical exposures to different infectious diseases, and other types of events that may have impacted the state of our immune system. In the case of cancer, the immune setpoint determines how someone’s immune system will respond to the cancer cells and whether they can control the tumor.
“…the immune setpoint determines how someone’s immune system will respond to the cancer cells and whether they can control the tumor.”
How do we characterize an individual’s immune setpoint?
The most common approach is to measure the types of immune cells that are present in someone’s body and look at how those cells are behaving. Cytometry-based approaches have historically been the most common way to do that. We use mass cytometry to measure the expression of roughly 45 different proteins across hundreds of thousands of cells at the single-cell level. Some of those proteins help us identify different types of immune cells, while others give us insight into how those cells are behaving or functioning. It’s been a really powerful tool over the last decade to understand more about the human immune system and how it responds to different perturbations.
We also have technologies that similarly can measure gene expression at the single-cell level. Other types of analyses provide us with complementary information on the chromatin landscape of immune cells, the abundance of circulating proteins such as cytokines and chemokines, as well as T cell and B cell receptors expressed by someone’s adaptive immune cells. These are layers of information that we now have access to, which can give us additional insight into the state of someone’s immune system.
Not typically. There are other tools that doctors use to help decide whether a patient is likely to benefit from a drug. However, these approaches still leave a significant amount of uncertainty. For example, doctors currently look for specific mutations that correspond to the signaling pathways that therapies can target. The challenge is that cancers often find ways to escape by evolving and developing resistance. So, while a patient’s cancer might initially benefit from these drugs targeting a specific mutation, the effect may not be long-lasting.
In contrast to these targeted therapies, immunotherapies have the potential to activate immune cells that recognize cancer cells as foreign, and this can result in the formation of long-lived memory cells that protect against cancer recurrence for long periods of time. We have some clues as to which patients are more likely to benefit from immunotherapy, but often these responding patients are difficult to predict using the tools currently available to oncologists.
“…immunotherapies have the potential to activate immune cells that recognize cancer cells as foreign, and this can result in the formation of long-lived memory cells that protect against cancer recurrence for long periods of time.”
If that’s the case, what could be a better approach?
Most drugs are initially developed because the pathways that they target were thought to be important in cancer cells or in other types of cells within the local tumor microenvironment. As we learn more about what those drugs are doing in people and in mouse models, it has become apparent that many of them are acting outside of the tumor as well. So, we should really be thinking about interactions outside of the tumor that could be used to activate cells that have the potential to drive new immune responses. Understanding how immune responses outside the tumor associate with clinical response is a real opportunity to better identify those patients likely to benefit.
For example, one of the main types of immunotherapy to treat patients with solid tumors is called a checkpoint inhibitor. Many of these inhibitors block a protein called PD-1 or its ligand, PD-L1. Originally, it was thought that, how many T cells express PD-1, or how many cancer cells or myeloid cells express PD-L1, would be interpretable information that would predict efficacy. This turned out not to be quite as straightforward as we would have thought. For instance, scientists found that many patients who have high levels of PD-L1 don’t necessarily respond well to checkpoint inhibitors. Meanwhile, some patients who don’t have a high expression of PD-L1 respond well.
We’re still working to understand exactly why that is the case. But one of the things we’ve learned is that these checkpoint inhibitors are, at least in part, not only acting on cells that are in the tumor tissue, but also on cells outside of the tumor tissue, including cells in the lymph nodes. These peripheral cells can be activated outside of the tumor, circulate through the blood, infiltrate into the tumor, and kill cancer cells.
“…these checkpoint inhibitors are, at least in part, not only acting on cells that are in the tumor tissue, but also on cells outside of the tumor tissue, including cells in the lymph nodes.”
This suggests that looking only into the tumor tissue is limited because it doesn’t provide you with full insight into one’s immune responses. There is a real opportunity for immune monitoring or measuring the immune setpoint outside of the tumor to understand somebody’s baseline immune state.
Do you think immune profiling will change the way we treat cancer patients in the future?
The immune system provides us a unique opportunity to fight cancer because of its ability to adapt, to keep up with changes that take place in cancer. It clearly has the potential to be very powerful if we can figure out how to effectively harness it across all patients.
I think there are opportunities that we might be missing when we don’t think about important pathways or interactions outside of the tumor. We need to be thinking critically about the variability that exists across patients in their immune states and to what extent they’re likely to be able to mount an immune response to different types of drugs. I think it is clear that there will be great utility for these immune profiling technologies in tailoring treatment strategies for particular patients and in different disease contexts.
The field has made tremendous progress in this area over the last 20 years, and many patients are now experiencing the long-term, durable benefit of immunotherapies. There is a very real opportunity for us as a scientific and medical community to continue making advancements in this area to improve patient outcomes with the latest technologies available.
If you’re developing a drug that acts on the immune system, one of the surprisingly hard problems is figuring out exactly what part of the immune system your drug hits.
This seems a bit paradoxical. If you’re developing a missile, you shoot the missile at the target, and you know what the missile hits. The target, right?
Not so simple. In human biology, you might think your drug hits only “T” cells, but the drug might actually hit “B” cells. Well, what’s the problem with that?
The problem is hitting the wrong part of the immune system might lead to seriously bad side effects, or even death in extreme cases.
As a result, scientists have developed a technique called “immune profiling” to figure out what cells of the immune system a drug is reaching. Flow cytometry is the most widely used version of immune profiling. Flow cytometry allows you to look at 6-8 protein markers on cells simultaneously, which is helpful for identifying a single type of immune cell, like T cells for example.
Imagine you have a drug aiming to do “something” to T cells. For example, you have a drug that should increase the number of T cells. When you measure the immune state with an immune profiling tool, you should see an increase in T cells.
The problem is, by focusing just on T cells (or a small subset), you can miss many important cell types, like Myeloid cells and B cells, that your drug might be affecting.
The problem is, by focusing just on T cells (or a small subset), you can miss many important cell types, like Myeloid cells and B cells, that your drug might be affecting.
To illustrate this, let’s try to take on a similar problem: inflation.
Imagine you want to measure inflation in an economy. You need to look at prices, right? To see if the prices are going up, and at what rate.
Now, what if you went to Costco, and looked at hotdog prices? You would say there’s 0% inflation in the economy. Hotdogs have been $1.50 since 1985 at Costco.
Once you start measuring the price increases of milk, gas, coffee, and energy — you find out inflation is closer to 10%. So by measuring more prices in an economy, you get a better idea of what inflation really is.
The same concept applies to immune drug development. You measure more and more immune cells, you get a better picture of what your drug does to the immune system. And that’s where mass cytometry comes in. Rather than measure 6-8 markers on only T cells, you can measure ~44 markers across many immune cell types simultaneously. This ‘high-parameter’ immune profiling ensures you’re not basing the success of your drug program on only a subset of data.
Or, scientifically speaking, on the price of a Costco hotdog.
If you’re interested in high-parameter immune profiling for your drug, contact us to see how we can help you.
Associate Professor of Medicine, Department of Medicine, Division of Hematology, Oncology, and Transplantation at the University of Minnesota
The Research
My work centers around blood cancers. For many with conditions such as leukemia and myelodysplastic syndrome, the only potential cure is a stem cell transplant from a healthy donor. Even with the best possible match, these patients require immunosuppressive medications to prevent the new immune system from becoming overly activated. If the medications fail, the new donor immune system can attack the patient’s organs and tissues resulting in a life-threatening condition known as graft-vs-host disease.
For decades, scientists have been thinking about how to replicate the immune tolerance that develops during pregnancy as a model for transplantation tolerance – something I started to think about myself when I was pregnant with my first child 16 years ago. I was so interested in the potential for pregnancy hormones to calm an over-activated immune system that I conducted a phase I/II clinical trial of urinary-derived human chorionic gonadotropin (uhCG) – the main pregnancy hormone – for treatment of life-threatening GVHD (NCT02525029). Most, but not all, patients showed improvement with the treatment. I wanted to understand how the new donor immune systems did – or didn’t – respond to therapy with uhCG.
The Challenge
Although we knew what we wanted to study, we didn’t want to be too narrow in our focus. We wanted to leave some room for discovery. We tried scRNAseq but found our cryopreserved samples were too sticky and we couldn’t get good runs. The process also yields so much data – it can feel like too much to handle at times.
Experiments using basic flow cytometry suggested that Tregs were involved, but we wanted a deeper look at cell populations and to explore some hypothesis-driven biomarkers. Having struck out with scRNAseq and given the limitations of traditional flow cytometry, we needed another solution.
The Solution
Teiko came along at the right time. As soon as we saw that we would have the opportunity to start with a basic panel and customize some of the parameters, we knew this was what we needed. I could have envisioned needing to spend $50K building a basic panel, accounting for both reagents and staff time, so having this panel ready to go with a few open channels available for new markers afforded us the opportunity to get data turned around quickly.
“I could have envisioned needing to spend $50K building a basic panel, accounting for both reagents and staff time, so having this panel ready… afforded us the opportunity to get data turned around quickly.”
We of course had hopes, but we didn’t have any expectation that we would find anything, since human data is so messy. However, we were happy to see several very interesting hits, even with a stringent false discovery rate. We now have better insight to know what happens and why this therapy works.
I went into this project thinking that our field placed too much emphasis on T cells, but Teiko’s panel showed us that precisely targeting a specific T cell subset with the right therapy could have a major impact on patient outcomes. We also found several interesting signals in cell-bound and serum biomarkers. The answer to any complicated human disease is going to be more complicated than we like. This highly dimensional approach allows us to embrace that nuance and gives us more confidence moving forward.
Working with Teiko
Communication was seamless and quick. It was just like the Teiko team was across the hall. The analysis tools also helped us save 6 months or more, as I don’t have a PhD in bioinformatics, and those who do are often too swamped with requests to help.
“The analysis tools also helped us save 6 months or more…”
I especially liked working with Teiko’s webtool, which gave me the ability to play with the data. It felt really comfortable. We were all on the same team. Teiko felt like an extension of my research group.
Next Steps
I’m excited to see that clinicians have picked up on my research and are using uhCG to treat life-threatening acute GVHD today. I get messages and emails from people around the world with their experiences. The immune monitoring we performed with Teiko will be a huge plus for our phase II analysis. We often have to wait for weeks to get any insight into our patients’ trajectory, so any insights to change that path early in the disease course would be extremely powerful. The immune system is so complicated, and the reasons behind response to GVHD therapy poorly understood. Teiko helped us demystify at least a piece of the puzzle, and we look forward to more collaborations in the future.
Update!
This customer spotlight was originally posted in January 2023. In August 2023, Dr. Holtan published her work, including data generated by Teiko, in the journal Transplantation and Cellular Therapy. In February 2024, Dr. Holtan began her new role as the Chief of Blood and Marrow Transplantation, Professor of Medicine at Roswell Park Comprehensive Cancer Center.