“I have a 13 marker panel that analyzes T-cells. And my drug just hit the T-cells, why bother looking at any other immune cell types, like B cells, or NK cells? Even if those other cells are affected, I don’t know how to interpret those results.”
The reason is: those extra subsets might predict the difference between success and failure for a drug.
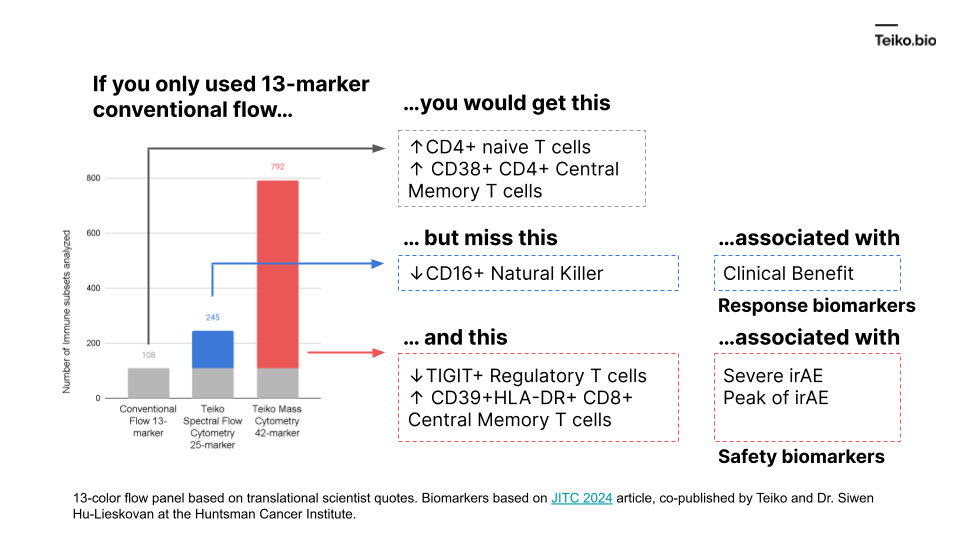
More to the point, if we took a conventional flow panel, you get up to ~108 subsets with a 13-marker panel, almost exclusively T cells. Using mass cytometry, with a 42-marker panel, you get to 792. With spectral flow, it’s around 245. This diagram shows what is missed by the lower-parameter methods. And these are cell subsets we ourselves have found in our own work and collaborations, associated with either clinical benefit, severe immune-related adverse events or peak toxicity.
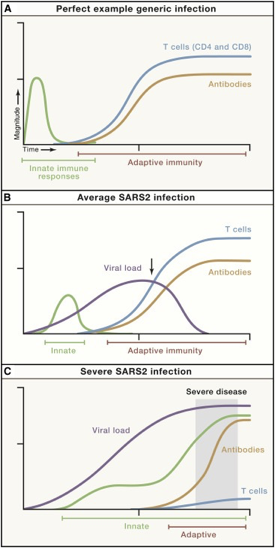
We know there is a “characteristic” time-series curve associated with clearing infections, like COVID. It would be difficult for a drug developer to analyze a “productive” immune response if whole curves were missing. For example, imagine tracking one curve, like the antibodies. If you tracked just antibodies, you could be misled into thinking someone had an average COVID infection or generic infection.
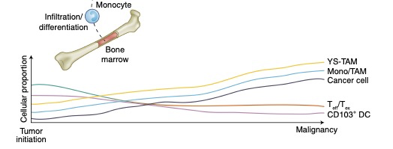
There is good reason to believe this sort of curve is true in cancer immunology. To that point, this is a nice time-series diagram from Nature Medicine of different cell types in the tumor microenvironment. The authors summarized it well: “understanding what cell types can be modulated and when may enable the next biggest improvements in immunotherapy.”
These distinct subtypes are not of academic interest: these drive real-world responses.
In this live webinar, Carlos Medina, Director of Product Management, and Will Chronister, Senior Computational Scientist, demonstrate how the newly redesigned TokuProfile Web can be used to answer critical research questions. This live demo will uses a real-world customer dataset, graciously provided by Dr. Shernan Holtan, Associate Professor at the University of Minnesota.
About the Speakers
Prior to Teiko, Carlos Medina completed his PhD training in Immunology at Stanford University in the laboratory of Dr. Paul Bollyky. There, he investigated the impact of the tissue extracellular matrix on regulatory T cell subsets in autoimmune diabetes and allergic asthma. Carlos has extensive experience in cytometry and immune cell profiling across a wide range of disease models.
Prior to Teiko, Will Chronister completed his PhD training in Biochemistry and Molecular Genetics at the University of Virginia. There, he investigated brain somatic mosaicism using single cell analysis and whole genome sequencing. Following this, he held roles as a Postdoctoral Fellow at the La Jolla Institute for Immunology and then as a Scientist, Bioinformatics at Fate Therapeutics before joining Teiko in early 2023.
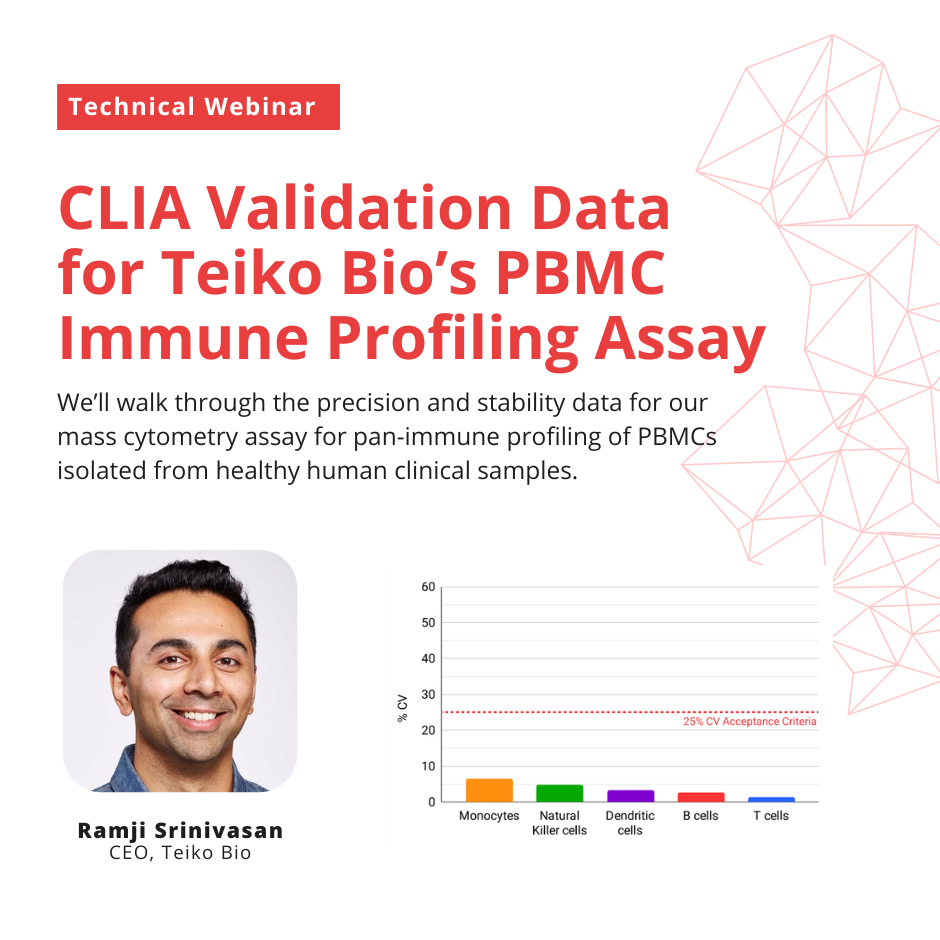
In this live webinar, Ramji Srinivasan, cofounder and CEO of Teiko Bio, will walk through the precision and stability data for our mass cytometry assay for pan-immune profiling of PBMCs isolated from healthy human clinical samples.
About the Speaker
Before Teiko, Ramji was Cofounder, CEO and Chairman of Counsyl, a women’s health genetic screening laboratory. Counsyl screened over 1M prospective parents, mothers-to-be and women at risk of hereditary cancer. In 2018, Counsyl was acquired by Myriad Genetics, Inc for $375M in cash and stock.
Ramji earned a B.S. in computer science and an M.S. in financial mathematics, both from Stanford University. Ramji also attended Stanford’s Graduate School of Business before dropping out to start Counsyl.
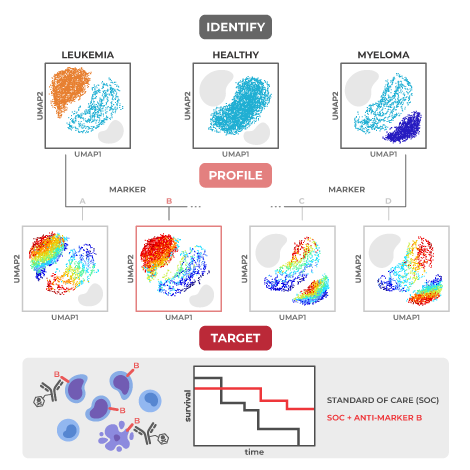
Many blood cancer studies today use immune profiling detection platforms that simply count the number of cancer cells, without providing any detailed information about their characteristics or interactions with healthy immune cells. This is where mass cytometry comes in – with the ability to evaluate over 40 protein markers per cell across hundreds of thousands of cells per blood sample1, it provides high-dimensional data that researchers can use to make crucial therapeutic discoveries.
Here, we highlight six recent key discoveries made using mass cytometry across a wide range of blood cancers including acute myeloid leukemia (AML), acute lymphoid leukemia (ALL), large B cell lymphoma, and multiple myeloma. With this powerful tool, researchers have uncovered new mechanisms of cancer relapse after chemotherapy, identified predictive biomarkers of response, and disentangled the role of non-cancerous immune cell populations in blood-based cancers.
High rate of dysfunctional NK cell development predicts poor outcomes in acute myeloid leukemia (AML)
Published in PNAS in 2021, Chretien et al. used two ~30 marker mass cytometry panels to characterize ‘dysfunctional’ natural killer (NK) cells overrepresented in newly diagnosed AML patients relative to healthy controls. This ‘dysfunctional’ NK population lacks expression of CD56, a marker highly associated with NK function, but expresses CD16, a crucial marker for antibody mediated killing by NK cells (CD56-CD16+).2 Importantly the cytotoxic killing potential of these cells, measured by degranulation in response to target cells, is reduced.
The authors found that having a higher percentage of these CD56- CD16+ NK cells at diagnosis was associated with poor clinical outcomes, lower overall survival, and a reduced likelihood of living free from disease complications (event-free survival). High dimensional analysis of single-cell protein expression by mass cytometry showed that these cells have lower expression of five activating receptors important for NK cytotoxic function: NKp30, NKp46, NKG2D, DNAM-1, and CD96.
Using an algorithm to analyze developmental pathways, the authors were able to identify a branching-off point where normal, mature NK cells diverge to become these dysfunctional NK cells. Future therapeutics targeting NK cells at this developmental stage may restore developmentally mature, functional NK cell populations for patients with AML, and thus likely improve clinical outcomes.
AML FLT3-ITD mutation and chemotherapy response: Why cytarabine might not be the best option
A study by Rörby et al. published in late 2021 used mass cytometry to approach the question: how does PKC412 synergize with a current standard chemotherapy regimen to produce good responses in AML patients?3 PKC412 is a newer anti-cancer drug, also called midostaurin, that improves overall survival for AML patients treated with a standard chemotherapy regimen consisting of daunorubicin and cytarabine. In 2017, it received approval by the US Food and Drug Administration (FDA) for use in patients with newly diagnosed FLT3-mutated AML, which is a common mutation affecting a third of AML patients that carries a poor prognosis. The researchers wanted to parse out the mechanism behind PKC412’s synergy with standard chemotherapy in order to potentially achieve higher clinical response rates by boosting complementary pathways and eliminating antagonist ones.
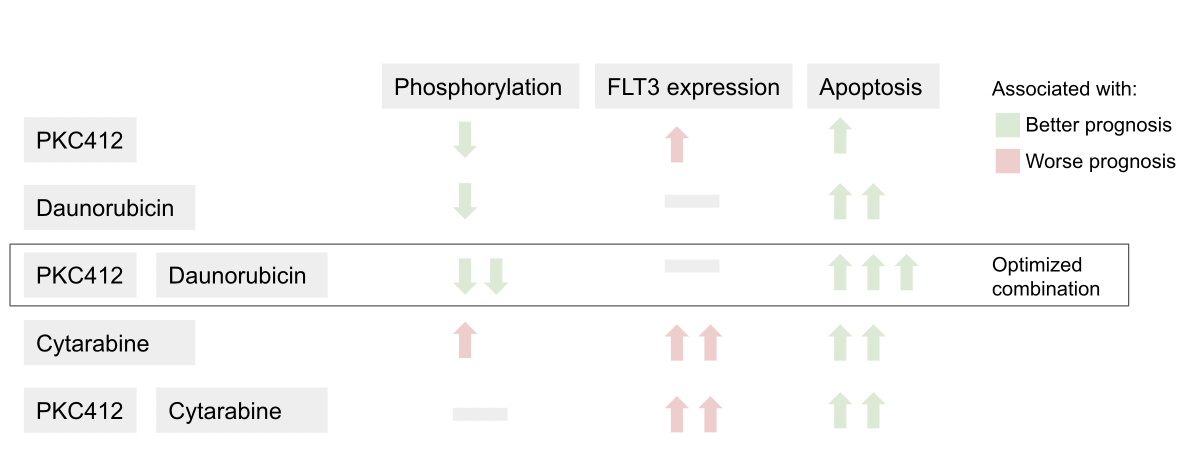
To tease out the impact of PKC412 on each component of the conventional treatment regimen, Rörby et al. used a 37-marker mass cytometry panel to evaluate the effects of various combinations of PKC412, daunorubicin, and cytarabine on intracellular signaling.
Summary of the effects of each drug combination on cell state
The authors found that daunorubicin works in concert with PKC412 to reduce phosphorylation (the addition of a phosphate group), a process that is necessary for molecular signaling cascades.3 In contrast, cytarabine increases FLT3 cell membrane receptor expression and intracellular signaling that reverses the activity of PKC412. These findings suggest that chemotherapeutic regimens without cytarabine, such as daunorubicin plus PKC412, may be more effective in treating the many AML patients who carry the FLT3-ITD mutation.
A combinatorial biomarker is a better predictor of response to anti-CD22 than CD22 expression alone in acute lymphoblastic leukemia (ALL)
With standard of care, around 90% of pediatric acute lymphoblastic leukemia (ALL) can be cured, but there is still around 10% of pediatric patients with relapsed or refractory (R/R) disease that remain resistant to treatment.4 A new drug that shows great potential to treat those with R/R ALL is Inotuzumab ozogamicin (InO), a CD22-directed antibody-drug conjugate. Although research from the Children’s Oncology Group and others suggested that resistance to InO might occur via reduced CD22 protein expression or density on the cell membrane, biomarkers for response to InO treatment had never been directly investigated.5
Diaz-Flores et al. used mass cytometry to evaluate whether the expression of any combination of 35 rationally selected protein antigens was associated with treatment response to InO.4 The proteins selected included cell surface markers, intracellular signaling molecules, and anti-apoptotic (cell survival) proteins that prevent programmed cell death, as well as other markers known to prevent cancer (so-called tumor suppressors) or resist drug exposure. After comparing antigen expression at diagnosis to changes in antigen expression after one and two cycles of treatment using a high-dimensional tumor cell-community clustering algorithm, the researchers were able to identify important combinatorial biomarkers predicting response to treatment.
The study authors identified the antigens that played the greatest role in distinguishing between complete and partial responder patient groups. Out of the handful of antigens identified, the most important discovery from the study was that low levels of CD22 had to be coupled with high levels of Bcl-2, an anti-apoptotic protein, to predict poor response to treatment. Low levels of CD22 alone could not predict poor response. These results suggested that the effects of InO, a drug that targets CD22, could possibly be improved by combining it with a drug to inhibit Bcl-2.
Exhausted NK cells hold the key to Daratumumab resistance in multiple myeloma (MM)
A study by Verkleij et al. used both flow and mass cytometry to evaluate the cellular response to the drug Daratumumab (DARA) in both newly diagnosed and relapsed/refractory multiple myeloma (R/RMM) patients.6 DARA, as part of a chemotherapy regimen, has been a promising treatment for R/RMM, with another study showing an improvement in complete response by 10% with the addition of DARA to a standard chemotherapy regimen.7 In this study, Verkleij et al. analyzed over 30 patient bone marrow and peripheral blood samples at baseline and at relapse using a mass cytometry panel with 39 surface and intracellular markers.
The authors found greater numbers of NK cells with an exhausted phenotype (higher frequency of TIM-3 expression and lower frequency of CD16 expression) in non-responding patients compared to responding patients at baseline, which was also seen in patients who relapsed. NK cells with an exhausted phenotype no longer carry out their normal characteristic functions such as the release of inflammatory signals or the ability to kill cancer cells. Patients with poor clinical outcomes also had greater numbers of both NK and T cells with an exhausted phenotype.
To determine whether resistance to DARA was due to NK cell exhaustion rather than a change in the multiple myeloma cancer cells themselves, the authors took cancer cells from patients who developed resistance to DARA and combined them with NK cells from healthy donors plus DARA treatment. They saw that DARA resistance was overcome by the addition of healthy NKs, suggesting that patients resistant to DARA may benefit from targeted reinvigoration of NK cells so they can destroy cancer cells again. This insight into the key role of NK cell activity was made possible by large-scale immune profiling through mass cytometry and is broadly applicable to situations where the target immune cell is initially unknown.
Tracking the success of CAR T cell therapy in MM with peripheral blood CD8+ T cells
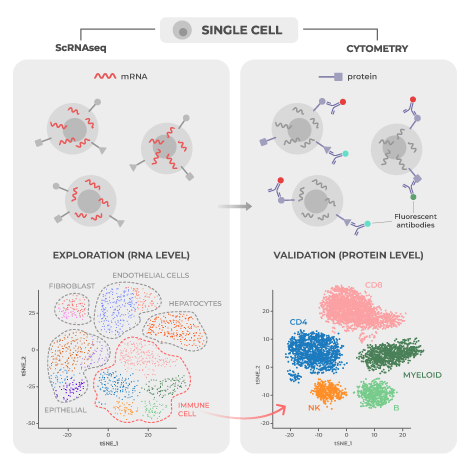
Another promising treatment for R/RMM is B cell maturation antigen (BCMA) CAR-T cell therapy, which involves genetically engineering a patient’s T cells so that they respond more forcefully to combat cancer cells. While many patients respond well to therapy, the response can be quite variable both in terms of initial effectiveness and in the duration of benefit. To explore variables that predict how patients will respond to BCMA CAR-T cell therapy, Melnekoff et al. conducted a study assessing single-cell transcriptomic and proteomic data from bone marrow (which is the tumor microenvironment in multiple myeloma) and peripheral blood samples using mass cytometry and single-cell RNA sequencing (scRNA-seq).8, two complementary technologies.
Using a mass cytometry panel of 39 cell markers, study authors analyzed 3.5 million peripheral blood mononuclear cells (PBMCs) from 11 patients treated with BCMA CAR-T cell therapy. Analysis of samples taken from peripheral blood and the bone marrow tumor microenvironment at baseline revealed that there were distinct cell population markers distinguishing good responders from poor responders, with responders having greater percentages of CD8+ T cells and lower percentages of CD14+ monocytes in both peripheral blood and bone marrow and lower NK cell population percentages in peripheral blood.
These same population changes were also observed over time in response to expansion of CAR-T cells in patients. Comparing week 0 to week 4 on CAR-T therapy, non-engineered CD8+ T cell numbers increased while CD14+ monocyte numbers decreased. The non-engineered CD8+ T cells were found to be exhibiting a so-called “effector-memory” phenotype that enables an immediate robust immune response at the site of contact with the disease-carrying cells. These shifts reverse when a relapse on CAR-T therapy occurs. CD14+ monocyte numbers level off or increase and CD8+ T cell numbers decline. Melnekoff et al. concluded that a certain class of immunomodulatory drugs called immunomodulatory imide drugs might increase the effectiveness of CAR-T therapy by increasing natural CD8+ T cell numbers.
A unique population of post-infusion CAR Treg cells identify patients resistant to CD19-CAR therapy
Treating diffuse large B cell lymphoma (DLBCL) patients with axi-cel, a chimeric antigen receptor (CAR) T cell therapy targeting CD19 (an important B cell biomarker) has proven to be difficult, with lymphoma continuing to progress in around 60% of patients and neurological toxicity affecting two-thirds of patients.9 Biomarkers connected to poor disease control and neurotoxicity have not been well characterized. For this reason, Good et al. conducted a study to investigate circulating CAR T cells in 32 patients treated with axi-cel using mass cytometry to profile 37 proteins per cell.
The researchers found two metaclusters associated with complete response, both of which were positive for CD57 and expressed inhibitory proteins, such as PD-1, at lower levels.9 They also found a metacluster of CD4+Helios+ CAR T cells 7 days post-infusion that correlated with disease progression and diminished neurotoxicity. These cells expressed high levels of CD25, CTLA4 and TIGIT, a phenotype characteristic of immunosuppressive regulatory T cells (Tregs). The authors validated their findings in a prospective cohort analysis of 31 DLBCL patients treated with axi-cel.
This study demonstrates the usefulness of mass cytometry to find biomarkers correlated with treatment response, disease progression, or toxicity in DLBCL patients. The discovery of a unique population of CAR Treg cells associated with disease progression and reduced neurotoxicity may allow future researchers to specifically manipulate these cells before or after infusion to promote anti-tumor effect or lower neurotoxicity.
Future of high-dimensional immune profiling for blood cancers
In addition to the examples highlighted earlier, recent research presented at the December 2022 American Society of Hematology Conference investigated many other blood cancers, including follicular lymphoma and chronic myeloid leukemia. Other ongoing studies focus on AML patients with adverse cytogenetics and drug resistance in patients with other blood cancers like DLBCL and multiple myeloma.
Collectively, these studies showcase the capabilities of mass cytometry to identify peripheral immune biomarkers that can predict relapse and treatment response across a broad range of blood cancers. A recent pre-print by Kleftogiannis et al. does just this using a combination of mass cytometry and machine learning algorithms to identify predictors of survival in leukemia. The technology’s unique ability to profile both the patient’s tumor and immune cells at the single-cell protein level positions it as an excellent tool to unravel the mechanisms behind relapse and response. This deeper understanding of the disease can then inform the development of more effective treatment protocols and therapies.
Everyone has a distinct “immune setpoint” that determines the way they respond to diseases and treatments. Matthew Spitzer, Associate Professor at UCSF and scientific cofounder of Teiko Bio, explains how understanding each patient’s individual immune setpoint could be the key to maximizing cancer treatment efficacy.
What is an “immune setpoint” and how does it affect our responses to life-threatening diseases like cancer?
Each individual’s immune system is characterized by a unique homeostatic baseline, called the immune setpoint. The immune setpoint defines how our immune system behaves naturally, in the absence of a disturbance. This is based on our underlying genetics, historical exposures to different infectious diseases, and other types of events that may have impacted the state of our immune system. In the case of cancer, the immune setpoint determines how someone’s immune system will respond to the cancer cells and whether they can control the tumor.
“…the immune setpoint determines how someone’s immune system will respond to the cancer cells and whether they can control the tumor.”
How do we characterize an individual’s immune setpoint?
The most common approach is to measure the types of immune cells that are present in someone’s body and look at how those cells are behaving. Cytometry-based approaches have historically been the most common way to do that. We use mass cytometry to measure the expression of roughly 45 different proteins across hundreds of thousands of cells at the single-cell level. Some of those proteins help us identify different types of immune cells, while others give us insight into how those cells are behaving or functioning. It’s been a really powerful tool over the last decade to understand more about the human immune system and how it responds to different perturbations.
We also have technologies that similarly can measure gene expression at the single-cell level. Other types of analyses provide us with complementary information on the chromatin landscape of immune cells, the abundance of circulating proteins such as cytokines and chemokines, as well as T cell and B cell receptors expressed by someone’s adaptive immune cells. These are layers of information that we now have access to, which can give us additional insight into the state of someone’s immune system.
Not typically. There are other tools that doctors use to help decide whether a patient is likely to benefit from a drug. However, these approaches still leave a significant amount of uncertainty. For example, doctors currently look for specific mutations that correspond to the signaling pathways that therapies can target. The challenge is that cancers often find ways to escape by evolving and developing resistance. So, while a patient’s cancer might initially benefit from these drugs targeting a specific mutation, the effect may not be long-lasting.
In contrast to these targeted therapies, immunotherapies have the potential to activate immune cells that recognize cancer cells as foreign, and this can result in the formation of long-lived memory cells that protect against cancer recurrence for long periods of time. We have some clues as to which patients are more likely to benefit from immunotherapy, but often these responding patients are difficult to predict using the tools currently available to oncologists.
“…immunotherapies have the potential to activate immune cells that recognize cancer cells as foreign, and this can result in the formation of long-lived memory cells that protect against cancer recurrence for long periods of time.”
If that’s the case, what could be a better approach?
Most drugs are initially developed because the pathways that they target were thought to be important in cancer cells or in other types of cells within the local tumor microenvironment. As we learn more about what those drugs are doing in people and in mouse models, it has become apparent that many of them are acting outside of the tumor as well. So, we should really be thinking about interactions outside of the tumor that could be used to activate cells that have the potential to drive new immune responses. Understanding how immune responses outside the tumor associate with clinical response is a real opportunity to better identify those patients likely to benefit.
For example, one of the main types of immunotherapy to treat patients with solid tumors is called a checkpoint inhibitor. Many of these inhibitors block a protein called PD-1 or its ligand, PD-L1. Originally, it was thought that, how many T cells express PD-1, or how many cancer cells or myeloid cells express PD-L1, would be interpretable information that would predict efficacy. This turned out not to be quite as straightforward as we would have thought. For instance, scientists found that many patients who have high levels of PD-L1 don’t necessarily respond well to checkpoint inhibitors. Meanwhile, some patients who don’t have a high expression of PD-L1 respond well.
We’re still working to understand exactly why that is the case. But one of the things we’ve learned is that these checkpoint inhibitors are, at least in part, not only acting on cells that are in the tumor tissue, but also on cells outside of the tumor tissue, including cells in the lymph nodes. These peripheral cells can be activated outside of the tumor, circulate through the blood, infiltrate into the tumor, and kill cancer cells.
“…these checkpoint inhibitors are, at least in part, not only acting on cells that are in the tumor tissue, but also on cells outside of the tumor tissue, including cells in the lymph nodes.”
This suggests that looking only into the tumor tissue is limited because it doesn’t provide you with full insight into one’s immune responses. There is a real opportunity for immune monitoring or measuring the immune setpoint outside of the tumor to understand somebody’s baseline immune state.
Do you think immune profiling will change the way we treat cancer patients in the future?
The immune system provides us a unique opportunity to fight cancer because of its ability to adapt, to keep up with changes that take place in cancer. It clearly has the potential to be very powerful if we can figure out how to effectively harness it across all patients.
I think there are opportunities that we might be missing when we don’t think about important pathways or interactions outside of the tumor. We need to be thinking critically about the variability that exists across patients in their immune states and to what extent they’re likely to be able to mount an immune response to different types of drugs. I think it is clear that there will be great utility for these immune profiling technologies in tailoring treatment strategies for particular patients and in different disease contexts.
The field has made tremendous progress in this area over the last 20 years, and many patients are now experiencing the long-term, durable benefit of immunotherapies. There is a very real opportunity for us as a scientific and medical community to continue making advancements in this area to improve patient outcomes with the latest technologies available.
If you’re developing a drug that acts on the immune system, one of the surprisingly hard problems is figuring out exactly what part of the immune system your drug hits.
This seems a bit paradoxical. If you’re developing a missile, you shoot the missile at the target, and you know what the missile hits. The target, right?
Not so simple. In human biology, you might think your drug hits only “T” cells, but the drug might actually hit “B” cells. Well, what’s the problem with that?
The problem is hitting the wrong part of the immune system might lead to seriously bad side effects, or even death in extreme cases.
As a result, scientists have developed a technique called “immune profiling” to figure out what cells of the immune system a drug is reaching. Flow cytometry is the most widely used version of immune profiling. Flow cytometry allows you to look at 6-8 protein markers on cells simultaneously, which is helpful for identifying a single type of immune cell, like T cells for example.
Imagine you have a drug aiming to do “something” to T cells. For example, you have a drug that should increase the number of T cells. When you measure the immune state with an immune profiling tool, you should see an increase in T cells.
The problem is, by focusing just on T cells (or a small subset), you can miss many important cell types, like Myeloid cells and B cells, that your drug might be affecting.
The problem is, by focusing just on T cells (or a small subset), you can miss many important cell types, like Myeloid cells and B cells, that your drug might be affecting.
To illustrate this, let’s try to take on a similar problem: inflation.
Imagine you want to measure inflation in an economy. You need to look at prices, right? To see if the prices are going up, and at what rate.
Now, what if you went to Costco, and looked at hotdog prices? You would say there’s 0% inflation in the economy. Hotdogs have been $1.50 since 1985 at Costco.
Once you start measuring the price increases of milk, gas, coffee, and energy — you find out inflation is closer to 10%. So by measuring more prices in an economy, you get a better idea of what inflation really is.
The same concept applies to immune drug development. You measure more and more immune cells, you get a better picture of what your drug does to the immune system. And that’s where mass cytometry comes in. Rather than measure 6-8 markers on only T cells, you can measure ~44 markers across many immune cell types simultaneously. This ‘high-parameter’ immune profiling ensures you’re not basing the success of your drug program on only a subset of data.
Or, scientifically speaking, on the price of a Costco hotdog.
If you’re interested in high-parameter immune profiling for your drug, contact us to see how we can help you.
Research in the field of cancer immunotherapy increasingly demonstrates the value of studying circulating immune cells in peripheral blood to identify new therapeutic targets to enhance tumor-killing immune responses. Here we highlight a handful of impactful publications in this field and provide a strategy for implementing peripheral immune profiling in your research and drug development pipeline.
Fresh T cells from Blood Replenish Exhausted T Cells in Tumor to Sustain a Tumor-Killing Response
If tumor killing by immune cells happens at the tumor site,what is the role of the peripheral immune response in the effectiveness of immunotherapy treatments? Wu et al. address this important question in a Nature 2020 article.1 Cancer cells hide from immune cells using checkpoint proteins, such as PD-L1, that keep immune cell responses “in check.” Anti-PD-L1 monoclonal antibodies and others prevent cancer cells from doing this; they form a class of drugs known as immune checkpoint inhibitors.
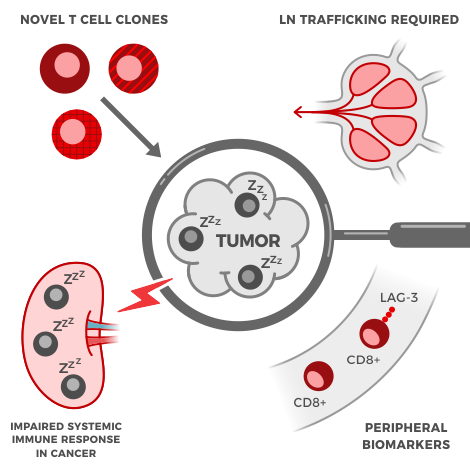
The researchers used deep single-cell sequencing of RNA and T cell receptors to analyze the characteristics of different populations of T cells and T cell receptors in tumors, normal tissue next to the tumor (normal adjacent tissue), and peripheral blood. Using these methods, the study authors were able to identify the location of targeted clonal expansion (replication of identical cells, called clones) of effector-like T cells, the specific subset of T cells that have direct anti-tumor activity. Targeted clonal expansion within peripheral blood predicted local clonal expansion both within the tumor and in normal adjacent tissue at the same time, which was associated with the drug working better.
Data both from this study and others indicate that non-exhausted T cells (T cells that are fully functional and active) and T cell clones that travel from the periphery to the tumor play a central role in patients’ ability to fight off tumors after receiving immune checkpoint inhibitors. Thus, identifying and analyzing tumor-killing T cells in peripheral blood samples is not only convenient but critical to drug discovery. Therapeutic breakthroughs may be missed if peripheral blood analysis is ignored.
Reinforcements Needed: Effective Therapy Requires Immune Cells from Outside the Tumor
Teiko Bio’s cofounder Matt Spitzer and colleagues have published multiple studies demonstrating the importance of the peripheral immune response in cancer biology. In these studies, the research was carried out using mass cytometry, an advanced technique that expands on flow cytometry technology by using metal-tagged antibodies. Given the distinct characteristics of the metals used, mass cytometry has the capacity to detect more than 40 cellular markers simultaneously.
Prior to the publication by Wu et al., work by Spitzer et al. provided evidence that the peripheral immune system is the source of a prolonged and sustained tumor-killing response in their 2017 Cell paper.2 Using mass cytometry, the study authors investigated immune activity in a mouse model of triple-negative breast cancer following treatment with either a successful or unsuccessful immunotherapy.
The investigators found evidence of immune activity throughout the mouse’s body, not just in the tumor microenvironment. During the period of tumor rejection, eight days after giving a successful therapy, only peripheral immune cells, such as those from draining lymph nodes, spleen, peripheral blood, or bone marrow, exhibited a higher level of activity and replication (production of new cells). Furthermore, a specific subset of peripheral CD4+ T cells arose that provided immunity against new tumors, and their numbers grew in mice who responded to therapy. This peripheral immune activation was specific to successful therapy, as the peripheral immune cells of mice given an ineffective therapy showed very few immune differences when compared to untreated mice.
Cancer’s Impact on the Immune System Goes Beyond Tumor-Killing
A 2020 study published in Nature Medicine by Allen et al. explored how cancer alters systemic immune response to infection.3 Eight mouse strains bioengineered to develop tumors across five tissue types were investigated. In all mice studied, cancer development caused marked changes in systemic immunity; similar findings were demonstrated using gene expression data of breast cancer patients from the Norwegian Women and Cancer Study. In the mice, the immune cell changes in peripheral tissues were distinct from those in the tumor microenvironment.
The presence of tumor in the mouse models weakened the immune response to infectious disease. This manifested in many ways, including decreased T cell activity to fight off infections from viruses or bacteria. Investigators discovered that T cell activity could be restored by supercharging the response of another type of immune cell, called the antigen-presenting cell. When tumors were surgically removed, the healthy baseline functioning of the entire immune system was reestablished. Antibody blockade of specific immune signaling molecules (IL-1 and G-CSF) alone prevented many of the negative tumor-induced changes to overall immune function. This shows the importance of these signaling molecules to how the immune system dynamically changes and adapts to its environment. Results from this study provide convincing evidence that dynamic restructuring of the entire immune system, both in terms of composition and function, occurs in response to cancer.
How the immune system interacts with different types of cancer is now being studied for its potential as a predictive biomarker of response to treatment. Evidence for specific immune cell types guiding cancer progression, both positively or negatively, continues to build. A 2021 study by Shen et al. published in Science Translational Medicine found that certain immune protein identifiers (one of which is called lymphocyte-activation gene 3 or LAG-3 for short) on specific T cells (CD8+ T cells) predicted which patients would respond to immune checkpoint inhibitors.4 The researchers used flow cytometry to evaluate many different immune cell markers and the results were confirmed in two different patient data sets, one with melanoma (188 patients) and another with urothelial cancer. Both melanoma and urothelial cancer patients that had low levels of the LAG-3 immune biomarker on their CD8+ T cells were much more likely to respond to treatment.
A 2020 review paper published in Nature Reviews Cancer by Bruni, Angell, and Galon provides an outline of the primary immune factors that lead to tumors growing or shrinking.5 The importance of how the immune cell interacts with tumors can be seen in how checkpoint inhibitors work. If a robust adaptive anti-tumor immune response does not already exist before treatment, checkpoint inhibitors will be ineffective. There are many different cancer types, each having its own distinctive interactions with the immune system with many moving parts. Given this complexity, the authors of the review suggest that being able to predict how cancer patients respond to treatment can be improved by evaluating multiple immune parameters instead of relying on just one.
What to Look For When You Don’t Know What You’re Looking For
An article published in Cell Reports in 2019 explored the power of mass cytometry to overcome investigator bias and ensure detection of unexpected cellular activities in clinical trials.6 These unforeseen activities might provide the key to a therapeutic breakthrough even for trials with limited sample sizes. The study authors created a standardized, comprehensive reference panel of 33 antibodies that covers all major immune cells subsets in the innate and adaptive immune system, while also quantitatively measuring markers of activation and immune checkpoint molecules in one assay.
The mass cytometry panel was able to categorize at least 98% of peripheral immune cells, with each cell population expressing four or more antigens. The strength of the technique was demonstrated in its ability to produce consistent results across two research centers and different sample types, including peripheral blood samples, metastatic lymph node samples, and tumor biopsies. The investigators were able to characterize disease-associated immune signatures following bone marrow transplantation in leukemia patients who developed graft-versus-host disease compared to those who did not using their standardized 33 antibody reference panel. This published work formed the initial foundation for Teiko’s TokuProfile base panel, which was later optimized to add up to 12 additional open channels for customization.
In summary, a growing body of evidence suggests that not only can studying immune system changes in peripheral blood in clinical trial cancer patients result in important insights , but peripheral immune responses are key to finding immunotherapy breakthroughs. High-dimensional techniques such as mass cytometry, with its ability to gather data on the entire immune landscape at once, are leading the charge and helping researchers find clinically relevant biomarkers today.
Being able to leverage the strengths and skill sets of a strategic partner can mean the difference between finding a therapeutic breakthrough in your research pipeline or not. Make the most of your time and resources by choosing an immune profiling partner who can advance your oncology, autoimmune, or infectious disease pipelines. Here are five things to look for when evaluating an immune profiling partner.
It may seem obvious, but producing high-quality, interpretable data requires knowledge, skill, and experience. Be sure your immune profiling partner has enough experience to perform quality work in a timely manner and can troubleshoot challenges that arise. Does your service provider understand the nuances of different cell types? The subtleties of manual gating? Gating and computational expertise in high [40+] dimensional immune datasets can mean the difference between finding and missing subtle signals in your data.
How can you judge expertise when scoping a new partnership? Ultimately, the proof is in the pudding. The scientific leadership of the organization should have a trail of high-impact publications in established peer-reviewed journals and demonstrate innovative ways of understanding and exploiting our immune system to treat disease. Their team should be experienced and confident enough in the “language” of their technical knowledge base to creatively expand and grow its potential versus someone who only conventionally applies what has already been done before.
Another consideration is the technology being used to complete the immune profiling. The technique should make use of latest advances in science but at the same time must be properly vetted through the scientific process to ensure consistency and accuracy over time.
For example, mass cytometry or cytometry time of flight (CyTOF) is a technique that employs antibodies coupled to isotopically pure metals to detect and measure more than forty cellular features with single-cell resolution. It builds on the technology of flow cytometry to maximize resolution and parameterization (the number of markers that can be detected in a single cell). At the same time, the technique has been tried and tested and widely validated through rigorous research since becoming commercially available in 2009. Over the years, new techniques like SCAFFOLD [Single-Cell Analysis by Fixed Force- and Landmark-Directed] have been developed to visualize complex mass cytometry data. Powerful informatics techniques to make use of all the information mass cytometry data has to offer have been developed over the years by leaders in the field. Look for service providers that have expertise in the nuances of these different tools.
Batch effects arise from non-biological factors that influence data results, masking the relevant biological data necessary to move the research project forward. By using a barcoding set methodology, separate samples can be grouped together and analyzed in one tube, minimizing the variation between sets, or batches, that can develop from uncontrollable technical fluctuations.1 Such technical variability can arise from slight changes in the calibration of equipment or in the implementation of experimental procedures, such as staining, that are unavoidable when each batch is analyzed.2
Equipment calibration fluctuations are detected and eliminated via normalization algorithms that are calculated based on the variation of standardized calibration control beads between batches, which would otherwise be identical.2 Likewise, the effects of slight differences in experimental technique, such as staining, are detected and eliminated using anchor, or reference, control samples.1,2 Technical and biological replicates applied to each batch are used as anchor samples. A single donor, cell line, or tissue sample could be used as an anchor sample depending on the details of the study and its objectives.1 By means of computer analysis, transformation factors are then calculated to normalize anchor sample variation between batches.2
Make sure your immune profiling company employs both instrument calibration controls and biological anchor samples to guarantee that data is normalized appropriately. Doing so ensures that biologically relevant information can be clearly detected and data between batches is comparable.
Use of anchor, or reference, samples, calibration beads, and normalization algorithms are part of the broader picture of quality control. Quality control must be implemented for all components of an experiment including the instrument, reagents, methods, and samples.3 Instruments should be checked daily to make sure they are functioning properly within specified parameters, using calibration beads and diagnostic checks. Reagents must be tested for reliable performance, and methods must be consistent and standardized. Excellent quality control demands expert-level technical proficiency and problem-solving skills that only come from advanced training and experience.
Quality control extends to the handling and processing of your biological samples as well. Biological specimen samples are precious, and it is critical that your immune profiling partner make every effort to ensure that they are handled properly to generate reliable data you can be confident in. This includes quality control measures at every stage of sample processing, including on arrival, following fixation, and during data acquisition.
Regarding the handling of samples, disease stage and treatment can affect blood and PBMC (peripheral blood mononuclear cell) viability and quality. Thus, a good immune profiling partner is one who has experience processing many different types of biological specimens (e.g. whole blood, PBMCs, dissociated tumor or tissue samples, tumor-infiltrating lymphocytes, and bone marrow aspirate) from a variety of sources (human, mouse, non-human primates) collected using a variety of techniques (fixed and frozen).
The complexity and volume of data from high dimensional single-cell analysis requires increasingly sophisticated computing technology. Many important informatics algorithms have been developed throughout the 2010s.
One of these is CLARA (Clustering LARge Applications) clustering for large cytometry datasets which allows the data to cluster into groups and can identify unique subsets that may be missed by conventional cytometry gating strategies. This can be paired with an algorithm like Cluster Identification, Characterization, and Regression (Citrus).7 This program enables detection of cellular characteristics associated with targeted outcomes, such as patient survival to identify statistically significant and biologically relevant biomarkers.
Another algorithm is called Single-cell analysis by fixed force- and landmark-directed (Scaffold) maps.7 It employs a technique known as force-directed graphs, where the amount of likeness between cells functions as an attractive force while groupings are repelled by a repulsive force. The power of this bioinformatics technique is its ability to provide a 2-dimensional reference map of the immune system with static landmarks that can be used for easy comparison between samples or conditions. Changes to the system can then be better interpreted in their proper context and evaluated in comparison to other research study outcomes.
You’ll want an immune profiling partner that is familiar with a diversity of bioinformatics pipelines and may have even been a part of their development and validation. Computational approaches continue to evolve and a partner with a strong foundation who is continuing to evaluate modern approaches will ensure confidence and longevity of your analysis.
Time is precious and an important part of goal setting. When you assess turnaround time, it is important to look for a company that will provide end-to-end support at every step of the process from data acquisition through delivery and interpretation of results. Most contract research organizations (CROs) will cover the data acquisition, but leave the first mile and last mile up to you and your busy team. Look for a company that will work hand-in-glove with your existing scientific team to devise a detailed outline of the exact project scope, deadlines, and deliverables necessary to achieve your goals.
Leveraging the skill and experience of the right immune profiling partner to scope your project could save you a great deal of time and expense in the long run by avoiding errors that would stall your project or force your team to go back to the drawing board. Many CROs will leave you with raw data and excel spreadsheets. Look for a partner that provides data analysis and interpretation to save your company critical time and resources that could be better spent elsewhere.
Where to go for help
Whether you’re in the final stages of evaluating immune profiling partners or just beginning your search, our team of Senior Scientists is available to help answer any questions in your consideration process. You can book a meeting directly on our Contact Us page.